

Avoiding pregnancy
Modern fertility awareness methods (FAMs) include all methods which are based on identifying the fertile time. The effectiveness of these methods relies on the accurate identification of the fertile time and the couple's ability to modify their sexual behaviour. FAMs cover a diverse range of methods: calendar-based methods, observation-based methods (using one or more indicators of fertility) and technology-based methods which include urinary hormone test kits and monitors. Lactational Amenorrhoea Method (LAM), a transitional method for breastfeeding mothers, is also viewed alongside FAMs (more on LAM at a later stage)
Couples who intend to use FAMs to avoid pregnancy must have the support of an experienced practitioner. Users either need to abstain from intercourse or use a barrier method consistently and carefully until they can identify the fertile time. Each woman’s menstrual cycle is unique and many factors can disrupt cycles making chart interpretation difficult or impossible. It normally takes about six months to become confident in the use of FAMs. It may take longer for women who have irregular cycles or at times of changing fertility such as after stopping hormonal contraception, during breastfeeding or approaching the menopause.
Who can use FAMs?
The majority of women can use FAMs for avoiding pregnancy provided consideration is given to the factors which may disturb the cycle and the indicators of fertility. Modern FAMs do not rely on regular cycles, but women who have irregular cycles or are approaching the menopause may find these methods more difficult to use.
In some circumstances a practitioner may suggest that FAMs are not ideally suited in view of personal circumstances. FAMs can be highly effective but they are dependent on the user. Women who have medical conditions which would make pregnancy a high risk may not be suited to FAMs. Those women who are taking prescribed drugs which are contraindicated in pregnancy should not rely solely on FAMs. FAMs do not offer any protection against STIs.
How effective are FAMs?
The effectiveness of FAMs relies on a number of variable factors: the chosen method and the reliability of the fertility indicators, the quality of instruction, the user's ability to observe the indicators and follow the guidelines, the age of the woman, the frequency and timing of intercourse and whether barrier methods are used during the fertile time. This explains why there is such a wide variation in effectiveness.
FAMs which use a combination of indicators are up to 99% effective when motivated couples are taught by experienced practitioners, and follow evidence-based guidelines. This means that about 1 woman in 100 will conceive in a year when using the method correctly. (Frank-Herrmann 2007)
If FAMs are not used according to instructions, more women will get pregnant. Typical use failure rates as high as 24 women in 100 are often quoted for these methods, but this includes women who have had no formal instruction, use a single indicator method or an unreliable calendar calculation.
Combining the indicators of fertility
It is assumed that anyone reading this section is already familiar with the Fertility Awareness section which provides an overview of the menstrual cycle and the fertility indicators temperature, secretions, cervical changes and calculations. Women who are using FAMs to avoid pregnancy should always use a combination of indicators. A double-check of at least two indicators is required to identify the start and end of the fertile time. The following information explains how the fertility indicators are combined to provide an effective family planning method. The indicators will be described in turn, followed by a description about how these indicators are combined. Comprehensive coverage of the fertility indicators and their use for avoiding pregnancy can be found in The Complete Guide to Fertility Awareness
First Indicator: Waking temperature
The first indicator of fertility is the temperature. Progesterone (from the corpus luteum) causes a slight increase in waking temperature - this is used to confirm ovulation. In order to detect the subtle change, the temperature must be taken on waking, at the same time each morning and after resting for at least three hours. The temperature reading must be clearly marked on a reliable recording system. Blank charts and instructions for use can be found in the download area.
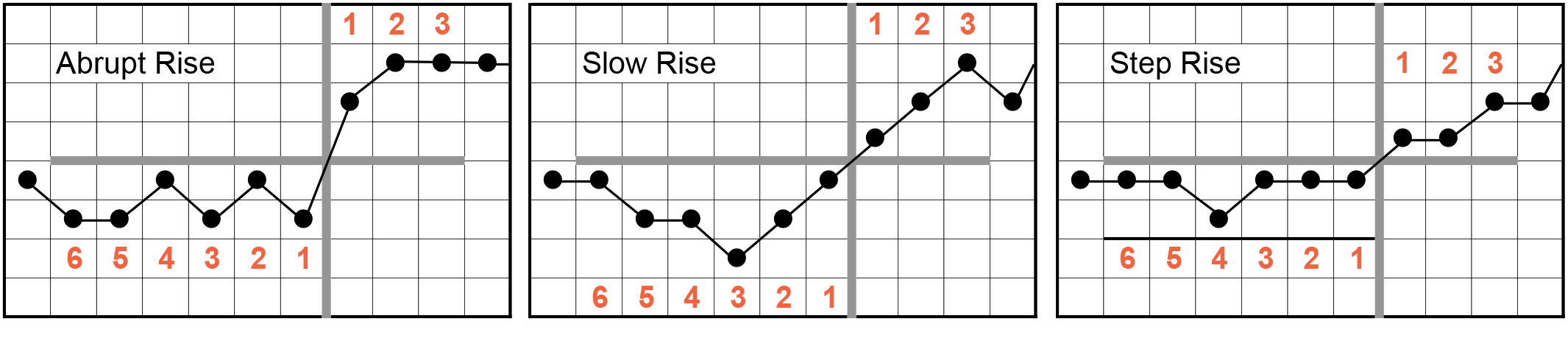
In a cycle where ovulation occurs (an ovulatory cycle), the waking temperature has two distinct levels. After the period the temperature stays at the lower level. Immediately after ovulation it rises by around 0.2 degrees centigrade to the higher level. The temperature remains at the higher level until the start of the next period: this is a biphasic cycle. The temperature rise helps to identify the end of the fertile time. There must be 3 undisturbed high temperatures above the level of the previous 6 low temperatures. The third high temperature must be a minimum of 0.2 deg.C. This is known as the 3 over 6 rule. To identify the appropriate temperatures, draw a horizontal line (cover-line) on the line immediately above the highest of the low-phase temperatures. Then draw a vertical line to form a cross dividing the low- and high-phase temperatures (see images below).
The temperature rise may occur abruptly, slowly or as a step-rise. There must always be 3 temperatures in the top right quadrant and 6 in the lower left. If the third high temperature is not at least 0.2 deg.C wait for a fourth high temperature which just needs to be above the cover-line.
Figure 1: Types of temperature rise
Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK 2016.
Disturbances affecting temperature
Many factors can cause disturbances in temperature. Body temperature is influenced by the circadian rhythm (the internal body clock): body temperature is at its lowest in the early hours of the morning (around 4.30 am) it then rises by approximately 0.1 deg.C. for every hour spent in bed. Changes in sleeping patterns, alcohol and drugs are common factors which disrupt temperature readings but with personal experience (and the help of a specialist FAM practitioner) these disturbances can often be managed. At times the disturbances are such that it is not possible to interpret the chart.
A disturbance may cause a temperature spike - a single recording which is 0.2 deg.C. or more above the one on each side. Alcohol, late nights, oversleeping, minor illness or stress are common causes of spikes. Sometimes there may be no apparent reason for a temperature spike. To mark the disturbance on the chart, circle the spike so that it can easily be seen and possibly discounted. One spike can safely be ignored when determining the six temperatures on the lower level, but where possible there should be an explanation for it. If there is more than one spike in the six low readings, the chart cannot be interpreted.
Figure 2 Temperature spike

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK 2016.
Example chart
Jo (not her real name) is 28 years old. She is in a committed relationship and planning pregnancy in about one year. In the meantime she is keen to learn more about her body and is using FAMs to avoid pregnancy. Jo's sixth chart will be used here as an example of a combined indicator chart. Her chart will be built up (for educational purposes) using a series of steps: first the temperature, then the changes in cervical secretions followed by changes in the cervix and finally a calendar calculation. The completed chart (figure 9) shows all the features of a combined chart.
Figure 6 demonstrates Jo's cycle length and temperature readings. The pink shading shows a five-day period with the next period starting on day 30, so this is a 29 day cycle. Jo has recorded her waking temperature every day. Note that her lie-in at the weekend (11th & 12th March) has caused disturbed readings. She has recorded a temperature spike on day 14 with no known cause for the disturbance. The temperature rises to the higher level on day 17. The third high temperature is at least 0.2 deg.C. above the low readings (note the hatched box to ensure that there is a 0.2 deg. C rise). One spike in the six low readings can be ignored. The 3 over 6 rule can be applied.
Figure 3 Section of Jo's combined chart showing a biphasic temperature

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK 2016.
In a biphasic cycle such as this the temperature usually remains at the higher level for 10-14 days before the next period starts - this is a normal length luteal phase. Sometimes this interval may be shortened - a short luteal phase. If the luteal phase is nine days or less, there may be insufficient time for implantation; which may be significant for women who are trying to conceive. Short luteal phases are not uncommon at times of stress and times of changing fertility. In a small percentage of cycles, there is no rise in temperature, the temperature stays on the low level until the next period starts – a monophasic chart may indicate that ovulation has not occurred.
Second indicator: Cervical secretions
The second indicator is the cervical secretions. The hormones estrogen and progesterone cause subtle changes in the secretions throughout the menstrual cycle. These secretions either encourage or impede sperm penetration. The images below show the cervix and sperm transport through its canal. The effect of estrogen is to facilitate sperm penetration through the cervical canal whilst progesterone blocks sperm penetration. Note the microscopic mesh-like structure - the thin mesh with wide gaps encourages sperm penetration whilst the the thick tight mesh prevents sperm penetration.
Effect of estrogen on cervical secretions

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK and the Institute for Reproductive Health, Georgetown University 2003.
Figure 4: Effect of estrogen on cervical secretions
When estrogen levels are low the thick white sticky secretions at the cervix give a feeling of dryness at the vulva (vaginal entrance). Sperm cannot easily penetrate through the cervical canal and are rapidly destroyed by the acidic vaginal environment. As the estrogen levels rise, sticky white secretions become visible at the vulva - this is the start of the fertile time. As ovulation approaches the secretions become wetter, more transparent and slippery, and they may be quite stretchy - sperm can move rapidly through these highly fertile secretions. (figure 4) The last day of the wetter secretion is known as peak day - this is usually close to ovulation. Peak day can only be recognised retrospectively on the day following peak when the cervical secretions have become sticky or dry again.
Effect of progesterone on cervical secretions

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK and the Institute for Reproductive Health, Georgetown University 2003.
Figure 5 Effect of progesterone on cervical secretions
Immediately after ovulation, under the influence of progesterone the cervical secretions become white, thick, and sticky again and form a sticky plug in the cervix, which blocks sperm penetration (figure 5). There will be a feeling of dryness at the vulva. This phase lasts until the start of the next period.
The cervical secretions can be recognised by, the sensation (feel) at the vaginal entrance, the appearance (look) describing the colour and the finger-test (touch) describing the consistency (see Planning Pregnancy Figure 2)
The secretions are observed throughout the day and recorded on the chart in the evening by shading in the appropriate box, indicating:
- the period (or spotting)
- dryness (no secretions seen or felt)
- early sticky white or cloudy secretions - these secretions are fertile
- wetter, more transparent, slippery stretchy secretions – highly fertile
The fertile time, based on cervical secretions alone, starts at the first sign of secretions (change from dryness) and lasts for three full days after peak day (last day showing the most fertile characteristics).
Figure 6 shows the cervical secretions recorded by Jo (sixth cycle of charting). The first secretions appear on day 10 and peak day is on day 15. The fertile time (based on secretions only) lasts from day 10 until day 18 (three days after peak).
Figure 6: Section of Jo's chart showing changes in cervical secretions

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK 2016.
The cervical secretions provide the best indicator of fertility for women who are planning pregnancy, however women who are using FAMs to avoid pregnancy should not rely on cervical secretions alone.
Third indicator: Changes in the cervix
The third indicator of fertility is the changes in the cervix. Not all women will wish to check their cervix, but for those who are comfortable with this practice, the cervical changes can give additional warning of the start of the fertile time. This may be of value for some women wishing to avoid pregnancy.
Just after a period, the cervix is low and easy to reach. It feels firm, and the os (cervical opening) feels closed. If you feel along the length of the cervix it feels quite long, and some women notice that it feels tilted to one side. It is generally quite easy to reach at this stage. Figure 7 shows the physiological changes in the cervix. As the estrogen levels rise, the cervix rises higher, becomes softer and shorter in length. It is now harder to reach with the finger-tip and may feel straighter (more central) in position. The cervical os feels slightly open. Notice the dotted line on the image which gives a guide to the height of the cervix. It takes almost a week for the cervix to change from its lowest closed position to its maximum height and openness. After ovulation, under the influence of progesterone, the cervix changes back within about 24 hours to its low, firm, closed, tilted position.
FIG 7: Changes in the cervix during the menstrual cycle

The changes in the cervix can be recorded on the chart as shown in Jo's chart (figure 8). The infertile cervix is represented by a solid black circle showing it to be firm and closed. The circle is placed low down on the baseline to represent it as lower in the vagina. A slanted line drawn below shows the tilt. The fertile cervix is represented by an open circle to show softening, with an inner circle showing that the cervical os is open. The circle is placed higher on the chart showing it to be higher in the vagina. A vertical line below shows the cervix straight in position.
In this example chart the first change in the cervix occurs on day 9 (softening). The cervix is high open and straight on days 13, 14 and 15. The cervix has returned to its low, firm, closed, tilted position by day 17. The fertile time (by cervix) starts at the first sign of any change from its low, firm closed, tilted position and ends after the cervix has returned to its infertile state and remained so for three days - so the fertile time according to cervical changes on Jo's chart lasts from day 9 to 19.
FIGURE 8: Section of Jo's chart showing changes in the cervix

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK 2016.
Anteverted or retroverted uterus
Most women have an anteverted uterus (that means that it points forwards slightly towards the pubic bone) but about 20% of women have a retroverted uterus (meaning that it points backwards slightly). This is usually quite normal and does not cause any problems with fertility, however it may affect the position of the cervix. With a retroverted uterus the cervix feels high in the pelvis at the infertile time and low at the fertile time (the reverse of the anteverted uterus). The cervix may point upwards slightly into the front wall of the vagina and the opening may be difficult to reach. It normally takes two or three cycles to learn to identify cervical changes.
It only takes a few seconds to check the cervix each day but new users are generally advised to delay checking the cervix until they have some experience of charting temperature and secretions. The changes in the cervix should never be relied upon as a single indicator.
Fourth indicator: Calculations
There is always a risk of pregnancy from intercourse in the early part of the cycle but a personalised calculation based on past cycle lengths can help to identify the start of the fertile time and improve the effectiveness of FAMs.
A woman who has an accurate record of the length of her last 12 menstrual cycles can use the S minus 20 rule. Estimate the shortest cycle length in the past year: e.g. if cycle lengths were 32, 27, 31, 30, 27, 29, 30, 27, 31, 28, 30 and 29 days, the shortest cycle (S) is 27 days. The calculation is: Shortest cycle minus 20 to give the first fertile day, so: 27 – 20 = 7. Day 7 is therefore the first fertile day in this example. The S minus 20 rule must be recalculated after each cycle to work on the length of the previous 12 menstrual cycles.
If a woman does not have a record of the length of her last 12 cycles, she can use the Day 6 rule. This allows intercourse up until day 5, with the fertile time starting on day 6. This rule can be applied from the 4th cycle provided that the first three cycles have been 26 days or longer. The Day 6 rule should be used until 12 cycle lengths have been recorded, thereafter the personalised S minus 20 rule can be used.
After a woman has completed 12 cycles of charting, she is considered an experienced user and can use her temperature readings to give a more personalised and accurate estimate of the start of the fertile time: Earliest temperature rise minus 7 = first fertile day. For example if, in the past year, a woman has recorded her first high temperature on days 14, 14, 16, 15, 16, 15, 16, 14, 15, 16, 14 and 14, her earliest temperature rise is day 14. (14 - 7 = 7) so day 7 would be her first fertile day. If in subsequent cycles, a temperature rise occurs on an earlier day, the calculation is adjusted accordingly. The calculation is always based on information form the most recent 12 cycles.
The stop bar
A calculation generally gives the earliest indication of the start of the fertile time, however a woman should always be vigilant for any change in the secretions or the cervix which may precede the day given by the calculation. A short vertical bar, the stop bar, can be drawn on the chart to show the start of the fertile time based on the Day 6 rule, S minus 20, or Earliest temperature rise minus 7. Couples need to understand that if they continue to have unprotected intercourse after the day designated by the stop bar they are at increasing risk of pregnancy. The fertile time starts at the earliest sign of change, whether from the secretions, cervix, or calculation — whichever comes first.
Figure 9 shows Jo's completed chart. The temperature, cervical secretions and cervical changes are combined. The information at the top of the chart shows that Jo's shortest cycle in the past 12 cycles was 27 days, so 27 - 20 = 7 (see stop bar between days 6 and 7)
The first sign of fertility by secretions is on day 10, the first change in the cervix is day 9, but the earliest sign of fertility is shown by the S minus 20 rule, so the fertile time starts on day 7. A double-check of temperature and cervical secretions is used to determine the end of the fertile time. The three high temperature must all be after peak day. In this example, peak day is on day 15, the temperature rises to the higher level on day 17 and all three high temperatures are after peak day (the third high temperature is at least 0.2 deg.C. above the low temperatures). The fertile time in Jo's sixth chart therefore starts on day 7 and ends on day 19.
Figure 9: Jo's completed chart showing the combined indicators (this chart can be downloaded here)

Copyright © Cecilia Pyper and Jane Knight in collaboration with FertilityUK 2016.
Disturbances affecting the chart
Any disturbance or change from normal routine should be noted on the chart. Some disturbances affect specific indicators of fertility whilst others cause more generalised disruption to the menstrual cycle. Disturbances include:
- Alcohol
- Late night, disturbed sleep, oversleeping (lie-in)
- Holidays, travel, particularly air travel and crossing time zones
- Shift work, particularly night shifts
- Daylight saving / changing the clocks
- Stress and anxiety
- Rapid weight loss or gain
- Intensive exercise
- Illness: acute or chronic
- Some bought or prescribed drugs and some herbal remedies
- Abnormal vaginal discharge
- Gynaecological conditions such as polycystic ovary syndrome (PCOS)
Each woman's response to disturbances will vary and some disturbances will be more prolonged than others. It may not be possible to interpret disturbed charts.
Fertility apps
Online charting systems and apps for mobile phones offer a convenient way to record and store fertility information, but this rapidly-expanding market is unregulated and lacks quality assurance. Some apps are simple period trackers but others allow the user to input different indicators of fertility. Theoretically apps which are based on the guidelines from the European Prospective Study (Frank-Herrmann 2007) may offer an effective method, but there have been no effectiveness studies to test this approach. A US team developed a tool to evaluate apps which claim to use evidence-based fertility awareness methods. See the FACTS web site for a rating of fertility apps marketed to avoid pregnancy. With the currently available evidence fertility apps cannot be recommended for avoiding pregnancy.
Further information and downloads
Fertility awareness charts and instructions for use can be accessed from the download area. You will also find examples of a completed chart, a "Getting Started" guide and a set of FAM guidelines. These resources are intended to supplement instruction from an experienced practitioner.